The architecture of crisis: Mapping the fractured line between the self and the system
A crisis is frequently conceived as an individual rupture, a moment of psychological fragility or emotional collapse. However, research in psychology and organizational sciences demonstrates that it extends far beyond the intimate sphere. Institutions themselves can enter a state of crisis when their customary mechanisms are no longer sufficient to cope with urgency, uncertainty, and threat.
Human life is never fixed in a state of absolute permanence. It is punctuated by sudden, destabilizing shifts and extraordinary challenges that call for singular interventions because they overwhelm an individual’s ordinary capacity to endure. This rupture is what we define as a crisis.
These critical tipping points reveal the fragile, moving boundaries of human experience. While some interpret these disruptions as purely negative suffering, others discover within them a profound crucible for growth and adaptation. Consider the abrupt termination of an employee. To the individual, this event may register as an existential collapse, a painful fracturing of stability, given that the occupation represents the primary means of survival and support for their family. From a different vantage point, however, this very rupture can serve as a catalyst, driving the individual to seek an alternative path that ultimately yields superior compensation, greater professional fulfillment, or better working conditions.
This conceptual framework represents a cornerstone of psychological research, particularly within organizational and occupational psychology. Its historical trajectory is remarkable, originating in classical medicine, migrating through political science, and finally embedding itself within contemporary sociological and psychological paradigms. The term is versatile, deployed with equal validity to describe medical emergencies, diplomatic standoffs, acute psychological distress, or broader societal upheavals.
The foundational moment for this concept within modern psychology occurred in 1944, when Erich Lindemann published his seminal study on acute grief following the catastrophic Cocoanut Grove fire in Boston. His insights provided the initial scaffolding for crisis theory. Lindemann characterized the crisis state as a natural biological and behavioral response to an overwhelming stressor, an event that simply outstrips an individual’s immediate psychological defenses. Consequently, the study of crises transformed into a central axis of clinical research, altering our approach to mental health and cognitive resilience.
Subsequently, Gerald Caplan established the rigorous methodological foundations of modern crisis intervention. His work was expanded by theorists such as Aguilera and Messick, who designed applied operational models to map the determinants of psychological collapse and paths toward resolution. Concurrently, Charles Hermann began integrating these principles into institutional environments, followed by scholars like Ian Mitroff, who mapped the structural dimensions of institutional shock, framing it as a predictable pattern that can be systematically managed and resolved. The concept has matured, analyzed through diverse theoretical lenses.
In our current era, the study of these disruptions has broken past the boundaries of individual psychiatric care. It now informs organizational governance and political science under the discipline of crisis management. Modern organizations no longer view institutional shocks as anomalous or rare anomalies. They recognize them as structural constants inherent to institutional life that require systemic, proactive stewardship. A crisis destabilizes the individual, inducing acute psychological pain, but it can just as easily threaten the continuity, integrity, and core objectives of a global enterprise.
Understanding the unique characteristics of this state is paramount to designing effective stabilizing measures. This duality raises profound philosophical and clinical questions. Should a crisis be treated as an acute mental illness requiring formal psychiatric treatment, or is it a normal adaptive response to an abnormal event? Furthermore, a definitional tension persists. Does the crisis reside within the fractured internal world of the individual, or is it a property of the broader systemic architecture? By revisiting these paradigms, this analysis explores the parameters of the crisis state, evaluating whether it manifests as an isolated pathological phenomenon or a systemic structural process, guided by the foundational work of Lindemann, Caplan, and Hermann.
🔗 Read also: From breaking point to breakthrough: How crises shape us
The etymological evolution of tipping points
The term “crisis” derives from the ancient Greek krisis, signifying a judgment, a critical choice, or a decisive moment, rooted in the verb krinein, meaning to separate, distinguish, or judge. This concept of a pivotal decision point underlies the contemporary usage of the word. The term found its initial definition within classical Greek medicine, where it denoted the absolute turning point of an illness, the fragile line separating recovery from death. Hippocrates utilized this framework to identify the critical phase of a clinical pathology. This historical legacy explains why the term remains deeply embedded in modern medical vernacular, seen in expressions like cardiac crisis or epileptic crisis. Within this clinical context, the crisis represents a volatile phase where the trajectory of an illness shifts rapidly toward either systemic regeneration or terminal decline.
In the political arena, a crisis represents a structural turning point for the state, demanding monumental executive decisions that will either restore systemic equilibrium or trigger an escalation of open conflict. This demonstrates that a crisis is never confined to individual somatic illness. It applies with equal force to corporate systems and social institutions.
The standard lexical definition describes a crisis as a prolonged period of difficulty, a state of profound collective or personal destabilization, or a sudden, severe worsening of a physical or psychological condition. The term encompasses multiple domains of human experience, including emotional, social, economic, or biological disruptions.
Synthesizing these elements reveals that the architecture of a crisis rests upon three fundamental dimensions.
The first is the temporal dimension. A crisis is not a permanent state of being, but an accelerated, condensed window of time characterized by intense pressure and urgency that demands immediate action.
The second is the structural imbalance. This manifests as a severe rupture in the system’s equilibrium, a state where traditional adaptive mechanisms and behavioral habits fail to function.
The third is the transformational dimension. The crisis state is inherently unstable and must resolve, leading either to systemic collapse or the emergence of a new, restructured equilibrium. This capacity for structural transformation makes the crisis an object of strategic management rather than a simple catastrophe, provided one understands its internal dynamics and behavioral feedback loops.
To grasp how a crisis functions as a psychological, cognitive, and organizational phenomenon, we must examine the primary theoretical frameworks that have shaped clinical practice and institutional policy. The following sections evaluate the psychological mechanics of individual trauma and the systemic dynamics of institutional collapse to provide a precise, integrated definition of this phenomenon.
The individual and the unforeseen: a clinical perspective
Erich Lindemann’s 1944 paper, “Symptomatology and Management of Acute Grief,” published in the American Journal of Psychiatry, transformed the scientific understanding of psychological shock. His work shifted the crisis paradigm from a subjective human experience into a structured domain of psychiatric theory, laying the groundwork for organizational applications.
Scholars widely recognize this study as the formal origin of scientific crisis theory. Gerald Caplan noted that modern crisis intervention models trace their lineage directly to Lindemann’s observations, while researchers like Parad and Parad defined it as the first systematic clinical investigation into acute emotional distress and its management.
Lindemann mapped the parameters of a crisis by analyzing the somatic and psychological expressions of grief in the survivors and families of the historic Boston nightclub fire. He demonstrated that acute grief is a distinct clinical syndrome characterized by a predictable constellation of psychological and physiological symptoms. This syndrome can erupt immediately following the trauma, manifest after a significant delay, become pathologically exaggerated, or appear entirely absent. Lindemann’s critical contribution was framing the crisis as a normal psychological response to an abnormal event rather than an inherent mental illness. However, it still induces a temporary collapse of executive functioning and daily coping skills. Through this work, the conceptualization of psychological shock transitioned from a static pathology toward a dynamic, time-limited process triggered by environmental trauma.
By documenting these acute behavioral responses, Lindemann challenged the prevailing psychiatric model of his era, which viewed psychological disorders as fixed structural defects within the personality. He reframed the crisis as a situational, transient state. An event only escalates into a true crisis when an individual’s established psychological defenses and coping strategies fail to contain the stressor. Not all adversity produces a crisis. The value of Lindemann’s model lies in framing the crisis as an actionable window for intervention, precisely because it is self-limiting in duration.
To prevent acute emotional distress from hardening into chronic psychological pathology, stabilizing measures must be built upon three principles.
- Interventions must be immediate.
- They must be tightly focused on the precipitating trauma.
- They must actively support and reinforce the individual’s executive ego functions.
Lindemann demonstrated that while a crisis is profoundly disruptive, it remains highly responsive to early psychological intervention and preventive care. Still, his analytical focus remained centered on the individual, emphasizing the subjective pain experienced in the wake of an isolated trauma.
Gerald caplan’s preventative model: heightened plasticity and the disequilibrium baseline
As public health and preventative psychiatry expanded across the United States, Gerald Caplan advanced the field by formalizing the models of psychological crisis. Extending Lindemann’s insights, he clarified that a crisis is a normal developmental or situational inflection point rather than a permanent psychological breakdown. Caplan developed the methodology of crisis intervention, demonstrating that these acute states represent windows of heightened psychological plasticity. They offer a unique opportunity for therapeutic stabilization before maladaptive behaviors solidify into chronic psychiatric disorders. Caplan observed that modern preventative psychiatry must deploy crisis intervention to stabilize individuals under acute environmental stress, thereby mitigating long-term psychological damage.
While Lindemann focused his research on the specific mechanics of acute bereavement, Caplan generalized the theory to encompass all critical life transitions and situational disruptions. He defined a crisis as a brief period of psychological disequilibrium in an individual confronted by a hazardous circumstance that presents a profound threat, an obstacle that they cannot escape and cannot resolve through their customary problem-solving strategies.
This framework identifies three core operational components.
- Psychological disequilibrium is the primary feature. The crisis breaks the individual’s habitual emotional baseline, generating severe internal tension, cognitive disruption, and a temporary inability to self-regulate behavior or affect.
- The hazardous event serves as the objective external trigger. A crisis does not develop in a psychological vacuum. It requires an identifiable environmental stimulus.
- The failure of existing adaptive resources marks the formal entry into the crisis state. When faced with an extraordinary challenge, the individual’s established coping mechanisms and psychological defenses prove inadequate, inducing an acute experience of helplessness.
A crisis is never caused solely by an external stressor. It emerges from the dynamic interaction between an individual’s internal cognitive resources and their external environment. However, this clinical paradigm treats the crisis as an isolated internal state, largely ignoring the institutional systems enclosing the individual. In modern society, where human behavior is mediated by complex organizations, psychological suffering cannot be decoupled from institutional architecture. When an environment breaks down, the system itself enters a state of crisis. Therefore, our analysis must transition from clinical psychology to systemic organizational theory.
🔗 Explore further: Burnout: When work pushes us to the edge
From ego to institution: the systemic pivot
Moving past clinical models focused on individual psychology, Charles Hermann introduced a structural alternative. He shifted the concept of crisis out of the psychiatric clinic and into the domain of organizational systems and decision theory. Hermann defined an organizational crisis as a situation that threatens high-priority goals of the decision-making unit, restricts the amount of time available for response before the situation is transformed, and surprises the members of the system by its occurrence.
This model represents an epistemological shift. An institutional crisis is no longer defined by subjective feelings of loss, but by a specific structural configuration characterized by three distinct variables.
- The first variable is structural threat. This occurs when leadership perceives an environmental shift as a direct challenge to the survival or core objectives of the organization.
- The second variable is severe time compression. Unlike routine operations, a crisis compresses the window available for strategic choice, exerting intense operational pressure on decision-makers.
- The third variable is situational surprise. This represents a failure of organizational anticipation. The sudden eruption of the event neutralizes standard operating procedures, inducing severe systemic stress.
To operationalize this model, Hermann constructed a theoretical framework known as “Hermann’s Crisis Cube,” which classifies institutional shocks based on the interactions of these three variables: threat, time compression, and surprise.
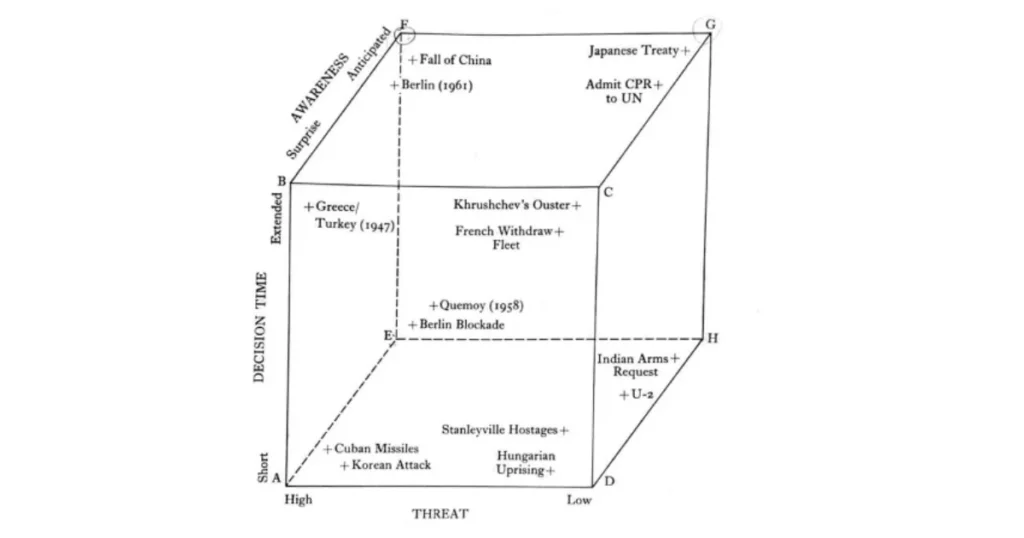
The structural architecture of this model maps three primary axes:
- The threat axis ranges from high systemic vulnerability to low operational risk.
- The decision time axis spans from acute short windows to extended planning horizons.
- The awareness axis moves from total situational surprise to complete operational anticipation.
The intersections within this space define eight distinct operational profiles, each representing a specific type of organizational emergency based on the severity of the three core variables.
Hermann’s model demonstrates that an institutional crisis is not merely an objective event, but a property of how executive leadership perceives and processes these three dimensions. If an organization utilizes strategic forecasting and scenario planning to transform a surprise event into an anticipated scenario, it shifts its operational profile away from the highly volatile danger zone into a manageable quadrant, even if the absolute level of structural threat remains elevated.
The fundamental tension between the clinical paradigm and systemic theory lies in their locus of definition. The clinical model views a crisis as a deeply painful, subjective psychological experience dependent on an individual’s cognitive appraisals. Conversely, systemic theory defines the crisis as an objective structural threat to the survival of an institutional system. The primary objective shifts from protecting an individual’s emotional well-being to rationalizing and optimizing the defensive response of the system.
The conceptual history of the crisis reveals a major evolution. It can manifest as an acute psychological disruption born from an individual’s appraisal of personal trauma, or it can develop as a severe, unanticipated threat to the equilibrium of an institutional system, demanding decisive governance across three operational constraints: threat, urgency, and surprise.
References
Aguilera, D. C. (1998). Crisis intervention: Theory and methodology (8th ed.). St. Louis, MO: Mosby.
Caplan, G. (1964). Principles of preventive psychiatry. New York, NY: Basic Books.
Hermann, C. F. (1963). Some consequences of crisis which limit the viability of organizations. Administrative Science Quarterly, 8(1), 61–82.
Koselleck, R. (2006). Le futur passé : Contribution à la sémantique des temps historiques. Paris: Éditions de l’EHESS.
Larousse. (s.d.). Dictionnaire de la langue française. Paris: Larousse.
Lindemann, E. (1944). Symptomatology and management of acute grief. American Journal of Psychiatry, 101(2), 141–148.
Mitroff, I. I. (1988). Crisis management: Cutting through the confusion. Sloan Management Review, 29(2), 15–20.
Nitten, V. (2004). La crise : Essai sur le concept et les dynamiques organisationnelles. Paris: L’Harmattan.
Orthodidacte. (s.d.). Dictionnaire d’orthographe et de grammaire françaises. Montréal: Druide.
Roberts, A. R. (2000). Seven-stage crisis intervention model: A road map to goal attainment, problem solving, and crisis resolution. Brief Treatment and Crisis Intervention, 1(1), 1–18.

Lhoussaine Ait Haddou
Occupational and Organizational Psychologist
Specialist in Organizational Psychology and Leadership
PhD Candidate at the Faculty of Letters and Human Sciences, Mohammedia, Hassan II University, Casablanca
Director of Psychi Life – Practical Psychological Services, Casablanca