Multiple sclerosis and psychomotor therapy
Relearning movement also means rebuilding confidence in the body itself. This is where psychomotor therapy has become an essential part of modern multiple sclerosis care.
Multiple sclerosis (MS) is now recognized as one of the most common chronic neurological diseases affecting young adults, primarily impacting individuals during a pivotal stage of personal, family, and professional development. The diagnosis often arrives at a time when people are actively planning their future, giving the disease a particularly profound psychological and existential impact.
In the collective imagination, MS is still too often reduced to visible motor impairment, embodied by walking difficulties or the use of assistive devices. However, this perception is deeply reductive. Multiple sclerosis is a complex, multifaceted, and progressive disease whose effects extend far beyond movement alone. Severe and disabling chronic fatigue, balance and coordination difficulties, sensory disturbances that may sometimes be diffuse, pain, cognitive impairments involving attention, memory, and processing speed, as well as emotional fluctuations, anxiety, and identity fragility all affect the individual across every dimension of functioning.
Beyond measurable symptoms, the disease profoundly transforms the relationship a person has with their own body. The body may become unpredictable, less reliable, subject to relapses, remissions, and fluctuating limitations over time. Actions that were once automatic can require heightened conscious control, fatigue imposes restrictions and renunciations, and body image may be altered by functional losses or the fear of worsening disability. MS is therefore not merely a disease of the central nervous system; it is also a bodily and subjective experience involving the psyche, emotions, and one’s relationship to the world.
It is precisely within this intersection between neurological impairment, embodied experience, and psychological adaptation that psychomotor therapy reveals its full relevance. As a discipline centered on the connection between body and mind, psychomotor therapy approaches movement not as a simple mechanical act, but as a global expression of the individual. It explores muscle tone and its regulation, coordination and balance, bodily perception, body image, the emotions associated with movement, and the sense of bodily identity.
In the context of multiple sclerosis, psychomotor therapy offers a sensitive, individualized, and evolving form of support capable of adapting to the fluctuations of the disease and the different stages of life. Its aim is to help individuals feel more at home in their bodies, regain reliable bodily reference points, preserve autonomy, and maintain a sense of continuity despite the transformations imposed by the illness.
This article therefore offers a clear, accessible, and scientifically grounded perspective on multiple sclerosis while highlighting the fundamental role of psychomotor therapy in supporting people living with the condition. Through a transversal approach, it seeks to demonstrate how psychomotor therapy represents an essential tool for quality of life, prevention, and support across all stages of life, from childhood to old age.
🔗Read also: Mental health begins in the body
From Charcot to modern neuroscience
Although descriptions suggestive of multiple sclerosis existed before the nineteenth century, it was the French neurologist Jean-Martin Charcot who gave the disease a true clinical identity. In 1868, he produced the first systematic description of MS by linking several clinical manifestations, including speech disturbances, intentional tremors, and nystagmus, to the presence of sclerotic plaques scattered throughout the central nervous system. This connection between clinical symptoms and anatomical lesions marked a foundational moment in the scientific understanding of the disease.
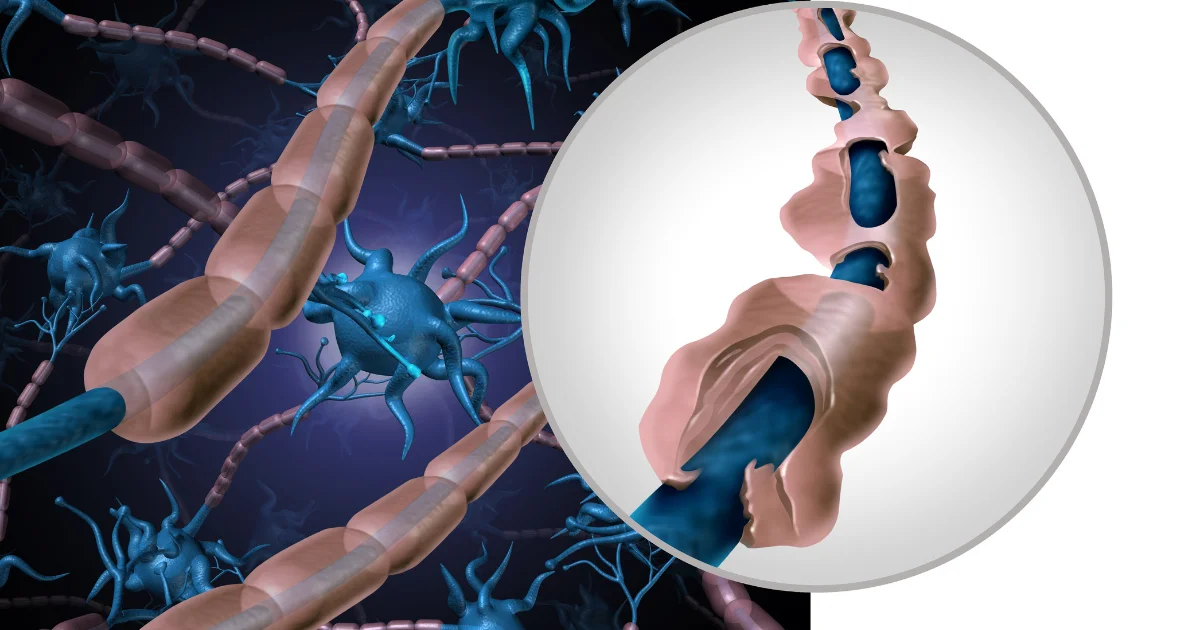
At the beginning of the twentieth century, advances in neuropathology made it possible to identify the destruction of myelin as well as the inflammatory processes associated with it. Gradually, MS came to be recognized as a chronic inflammatory disease with an autoimmune component involving mechanisms of demyelination and axonal degeneration.
The arrival of magnetic resonance imaging (MRI) in the 1980s represented a major breakthrough. For the first time, clinicians could visualize brain and spinal cord lesions, monitor their evolution over time, and improve both diagnostic precision and treatment assessment.
Beginning in the 1990s, the development of immunomodulatory and immunosuppressive treatments profoundly transformed the therapeutic landscape by slowing disease progression and reducing the frequency of relapses. At the same time, research increasingly focused on neuroprotection, remyelination, and brain plasticity, opening new perspectives for rehabilitation and functional recovery.
More recent studies have also highlighted the marked heterogeneity of multiple sclerosis. Several disease courses are now distinguished, each with specific clinical trajectories. This variability underscores the importance of personalized approaches that consider not only biological characteristics but also the functional, psychological, and social dimensions of the disease.
The history of multiple sclerosis therefore illustrates a gradual shift from a description centered on visible symptoms toward a multidimensional understanding integrating biology, imaging, immunology, and the lived experience of the patient. This evolution has fostered the development of multidisciplinary care approaches in which psychomotor therapy now occupies an increasingly important place.
🔗Explore further: From hysteria to science: The legacy of Jean-Martin Charcot
When the body becomes unpredictable
Multiple sclerosis is often defined as a neurological disease that disrupts the transmission of nerve impulses. Although accurate, this definition remains incomplete. MS does not affect only nerve fibers; it also transforms how a person inhabits their body, perceives their capacity for action, and experiences movement in everyday life. Understanding its full implications requires integrating perspectives from neurology, neuropsychology, and psychomotor therapy.
From a biological standpoint, MS is an autoimmune disease of the central nervous system. The immune system attacks myelin, the protective sheath surrounding nerve fibers, causing inflammatory lesions and progressive axonal degeneration. These lesions can appear in different regions of the brain and spinal cord, explaining the diversity of symptoms, including motor, sensory, visual, cognitive, and sphincter-related difficulties.
The disease particularly disrupts neural circuits involved in coordination, balance, and movement planning. When these networks are altered, movement becomes less fluid, more effortful, and sometimes uncertain. The brain attempts to compensate through neuroplasticity by recruiting other regions to maintain function. However, this compensation increases cerebral energy expenditure and contributes to central fatigue, one of the most common and often invisible symptoms of MS.
MS also alters sensorimotor loops that normally allow movements to adjust automatically. Actions that were once spontaneous may require more conscious control and greater reliance on attention and executive functions. Neuropsychological impairments frequently observed in MS, including slowed information processing and attentional or executive difficulties, interact directly with motor functioning. Walking in a complex environment or managing dual tasks therefore becomes significantly more demanding.
However, reducing MS solely to its neurological mechanisms would be insufficient. The disease is deeply rooted in embodied experience, in the subjective reality of living within one’s body. The unpredictability of relapses and symptom fluctuations often creates chronic uncertainty. This instability may lead to bodily hypervigilance, where individuals closely monitor their movements to avoid mistakes or falls, which in turn can increase muscular tension and reduce movement fluidity.
Fatigue particularly illustrates the interaction between brain, body, and psyche. It is a profound form of fatigue, often independent of physical exertion, affecting alertness, motivation, and motor precision. Psychomotor therapy therefore aims to improve energy management, encourage more economical movement patterns, and restore a sense of bodily security.
The disease also affects body image. Functional losses, motor limitations, or the use of assistive devices may weaken self esteem. In psychomotor therapy, bodily mediations such as relaxation, breathing exercises, sensory work, and expressive techniques seek to support bodily reintegration and restore continuity in the sense of bodily identity.
These biological, cognitive, and subjective dimensions constantly interact. Stress can intensify bodily tension and disrupt coordination, whereas a sense of safety can improve movement quality. Neuropsychomotor approaches are based precisely on this integrative vision in which brain, body, and psyche function together.
Viewing multiple sclerosis as a disease of both the body and embodied experience profoundly changes the therapeutic perspective. Neurological dimensions do not oppose subjective experience; they interact with it. Psychomotor therapy therefore occupies an essential place in care by helping individuals continuously rebuild their relationship with movement, their body, and their identity.
🔗Discover more: Living with Epilepsy: Why psychomotor therapy matters
Rediscovering the body through movement
Psychomotor therapy is grounded in a central idea: human movement is never purely mechanical. Every gesture involves the body, the brain, emotions, personal history, and the way individuals experience themselves within their own bodies. In multiple sclerosis, this approach is particularly relevant because the disease alters not only motor abilities but also the relationship to the body, effort, balance, and autonomy.
The psychomotor therapist therefore does not simply observe motor performance. They assess movement quality, muscle tone, balance, coordination, fine and gross motor skills, sensory integration, body image, and emotional regulation. This global perspective helps clarify how individuals adapt to their symptoms and how they continue to invest their body as a space of action, relationship, and confidence.
In MS, disturbances in muscle tone, spasticity, rigidity, fatigue, and postural instability directly influence movement fluidity. Psychomotor work seeks to refine bodily perception, encourage more economical adjustments, and reduce unnecessary tension. The goal is not merely to move better, but to regain a sense of safety in movement.
Balance and coordination are also central areas of intervention. These functions rely on the integration of visual, vestibular, and proprioceptive information. When these reference points become unreliable, individuals may lose confidence in their balance and reduce their mobility. Sessions therefore involve progressive situations designed to strengthen stability, prevent falls, and restore the exploratory dimension of movement.
Psychomotor therapy also considers the cognitive cost of action. In MS, walking, handling objects, or navigating complex environments can demand significant attentional resources, especially during dual task situations. Exercises may therefore combine movement, attention, rhythm, and planning in order to support motor automatization without exhausting the individual.
Another major issue concerns body image. Illness, functional limitations, or the use of assistive devices may alter self perception. Through relaxation, breathing work, sensory mediations, and expressive approaches, psychomotor therapy provides a space in which individuals can reconnect with a body that may sometimes feel unpredictable or unfamiliar. It helps maintain continuity between the perceived body, the lived body, and the acting body.
This perspective aligns with current scientific findings emphasizing the importance of movement, neuroplasticity, fatigue management, and quality of life in MS care. Interventions centered on adapted physical activity, balance training, body awareness, and mind body approaches highlight the value of active, personalized, and holistic care. Although research specifically focused on psychomotor therapy in MS remains limited, its principles fit fully within contemporary rehabilitation approaches that seek not only to treat deficits but also to support adaptive capacities.
Psychomotor therapy also varies according to different stages of life. In childhood, it aims to preserve developmental dynamics and support motor acquisition, sensory exploration, attention, and bodily confidence. Play occupies a central role because it allows children to work on balance, coordination, and emotional expression within a secure environment.
During adolescence, when the body becomes a central support for identity and social perception, MS may weaken self image. Psychomotor therapy then supports the transformations of both the pubertal body and the diseased body by encouraging body awareness, emotional regulation, pleasure in movement, and progressive autonomy.
In adulthood, when MS most commonly appears, the challenge is to preserve autonomy in everyday, professional, family, and social life. Work focuses on movement economy, fatigue management, tone regulation, coordination, and adaptation to real life situations. The objective is to help individuals develop a more conscious, secure, and sustainable way of moving.
In older adults, psychomotor therapy primarily aims to prevent psychomotor maladaptation, maintain balance, reduce fear of falling, and preserve the sense of bodily unity. Even when abilities decline, movement remains a space for experience, relationship, and dignity.
In every case, psychomotor therapy is part of an interdisciplinary approach alongside neurologists, physiotherapists, occupational therapists, neuropsychologists, and psychologists. Its specificity lies in bridging objective neurological data with the patient’s subjective experience. Its purpose is not merely to improve functions, but also to support the ability to inhabit one’s body, act with confidence, and remain an active participant in one’s own life despite the disease.
🔗Read also: How social media is reshaping our relationship with the body
When rehabilitation goes beyond movement
Multiple sclerosis cannot be reduced to visible motor symptoms alone. It progressively alters the relationship to the body, effort, space, and daily life. Walking, concentrating, maintaining balance, or managing fatigue may become activities requiring constant attention. This reality reminds us that the disease affects embodied experience as much as neurological functioning itself.
Within this context, psychomotor therapy occupies a unique position. Its goal is not only to improve motor function, but also to help individuals regain stable bodily reference points and greater confidence in action. Work on muscle tone, coordination, sensory perception, and fatigue management supports autonomy while also addressing the emotional and cognitive dimensions of the disease.
Therapy sessions become spaces for adaptation and experimentation. Individuals learn to better understand their limitations, conserve their energy, and develop new motor strategies compatible with everyday life. Regaining confidence in movement, reducing fear of falling, or rediscovering pleasure in movement already represent major achievements.
This approach also supports the specific challenges associated with each stage of life: motor development and bodily confidence in childhood, identity construction during adolescence, maintenance of autonomy in adulthood, and preservation of balance and quality of life in older age.
Current research in neurology and rehabilitation emphasizes the importance of active and holistic approaches in chronic disease care. Neuroplasticity, body awareness, and emotional regulation are now recognized as essential dimensions of treatment. Psychomotor therapy fits fully within this contemporary perspective by connecting neurological data with the patient’s lived experience.
Beyond rehabilitation techniques, psychomotor therapy ultimately offers another way of approaching chronic illness: not simply fighting limitations, but helping individuals preserve their ability to act, maintain a more peaceful relationship with their body, and sustain a meaningful quality of life.
References
Amato, M. P., Zipoli, V., & Portaccio, E. (2006). Multiple sclerosis related cognitive changes: A review of cross sectional and longitudinal studies. Journal of the Neurological Sciences, 245(1–2), 41–46.
Compston, A., & Coles, A. (2008). Multiple sclerosis. The Lancet, 372(9648), 1502–1517.
Dalgas, U., Stenager, E., & Ingemann-Hansen, T. (2008). Multiple sclerosis and physical exercise: Recommendations for the application of resistance, endurance and combined training. Multiple Sclerosis Journal, 14(1), 35–53.
Filippi, M., Rocca, M. A., Ciccarelli, O., De Stefano, N., Evangelou, N., Kappos, L., Rovira, À., Sastre-Garriga, J., Tintoré, M., Frederiksen, J. L., Gasperini, C., Palace, J., Reich, D. S., Banwell, B., Montalban, X., Barkhof, F., & MAGNIMS Study Group. (2016). MRI criteria for the diagnosis of multiple sclerosis: MAGNIMS consensus guidelines. The Lancet Neurology, 15(3), 292–303.
Fling, B. W., Motl, R. W., & Horak, F. B. (2020). Functional neuroplasticity in multiple sclerosis: The therapeutic potential of exercise training. Neurorehabilitation and Neural Repair, 34(7), 569–578.
Saad Chraibi
Psychomotor Therapist
• A graduate of Mohammed VI University in Casablanca, currently practicing independently in a private clinic based in Casablanca, Morocco.
• Embraces a holistic and integrative approach that addresses the physical, psychological, emotional, and relational dimensions of each individual.
• Former medical student with four years of training, bringing a solid biomedical background and clinical rigor to his psychomotor practice.
• Holds diverse professional experience across associative organizations and private practice, with extensive interdisciplinary collaboration involving speech therapists, psychologists, neuropsychologists, and other healthcare professionals.
• Specializes in tailoring therapeutic interventions to a wide range of profiles, with a strong focus on network-based, collaborative care.
• Deeply committed to developing personalized therapeutic plans grounded in thorough assessments, respecting each patient’s unique history, pace, and potential, across all age groups.